A New Cholesterol Problem?
When we talk about cholesterol and heart disease, most people have heard about LDL (“bad” cholesterol) and HDL (“good” cholesterol). But there is another cholesterol-related particle that deserves serious attention — especially in the Black community — and it rarely gets discussed. It is called Lipoprotein(a), or Lp(a) (pronounced “el-pee-little-a”), and it is one of the most significant inherited cardiovascular risk factors that disproportionately affects African Americans.
What Is Lipoprotein(a)?
Lipoprotein(a) is a type of lipoprotein particle in your blood. Think of it as a cousin of LDL cholesterol, but with an extra protein attached to it — a glycoprotein called apolipoprotein(a), or apo(a). This unique structure makes Lp(a) far more dangerous than standard LDL. On a particle-by-particle basis, Lp(a) is estimated to be roughly five to six times more atherogenic (artery-clogging) than regular LDL particles.
Lp(a) was first discovered by scientist Kare Berg in 1963, but it is only in the last decade or so that it has gained the serious medical attention it deserves. Here is what makes it particularly troubling: your Lp(a) level is almost entirely determined by your genes, not your diet or lifestyle. Up to 90% of your Lp(a) level is set by a gene called the LPA gene. You cannot walk it off, eat it away, or sweat it out at the gym.
Why Lp(a) Is a Major Issue for African Americans
Here is the reality that every Black American needs to know: African Americans have the highest Lp(a) levels of any racial or ethnic group in the world — higher than white Americans, higher than Hispanics, higher than East Asians.
In major multi-ethnic studies, Lp(a) levels in Black Americans have been found to be significantly elevated compared to every other group studied. In the landmark Atherosclerosis Risk in Communities (ARIC) study, which followed thousands of participants for 20 years, median Lp(a) levels were nearly three times higher in Black Americans (12.8 mg/dL) compared to white Americans (4.3 mg/dL). And critically, there was far greater variation among Black Americans — meaning some individuals had extremely high levels.
Research using data from a large California health system found that among patients tested, 62.6% of Black individuals had Lp(a) levels at or above 50 mg/dL — the threshold generally considered elevated — compared to only about 30% of Hispanic patients.
The Genetics Behind the Difference
Why do Black Americans have higher Lp(a)? The answer is largely genetic. Specific variations — called single-nucleotide polymorphisms (SNPs) — in the LPA gene explain most of the racial difference in Lp(a) levels seen in African Americans. These genetic variants have been carried forward through generations of people of sub-Saharan African ancestry.
There is one interesting twist worth noting. While Black Americans carry higher absolute Lp(a) levels, the heritability of Lp(a) — meaning how predictably it is passed from parent to child — is actually somewhat lower in African Americans than in white Americans. This makes the genetics slightly more complex in our community. Still, the bottom line remains: the absolute Lp(a) levels are highest in people of African ancestry, and that translates directly into real cardiovascular risk.
If your level is high, you have to be doubly sure you minimize your other risks by exercising, taking a statin, watching your diet, and controlling your blood pressure.
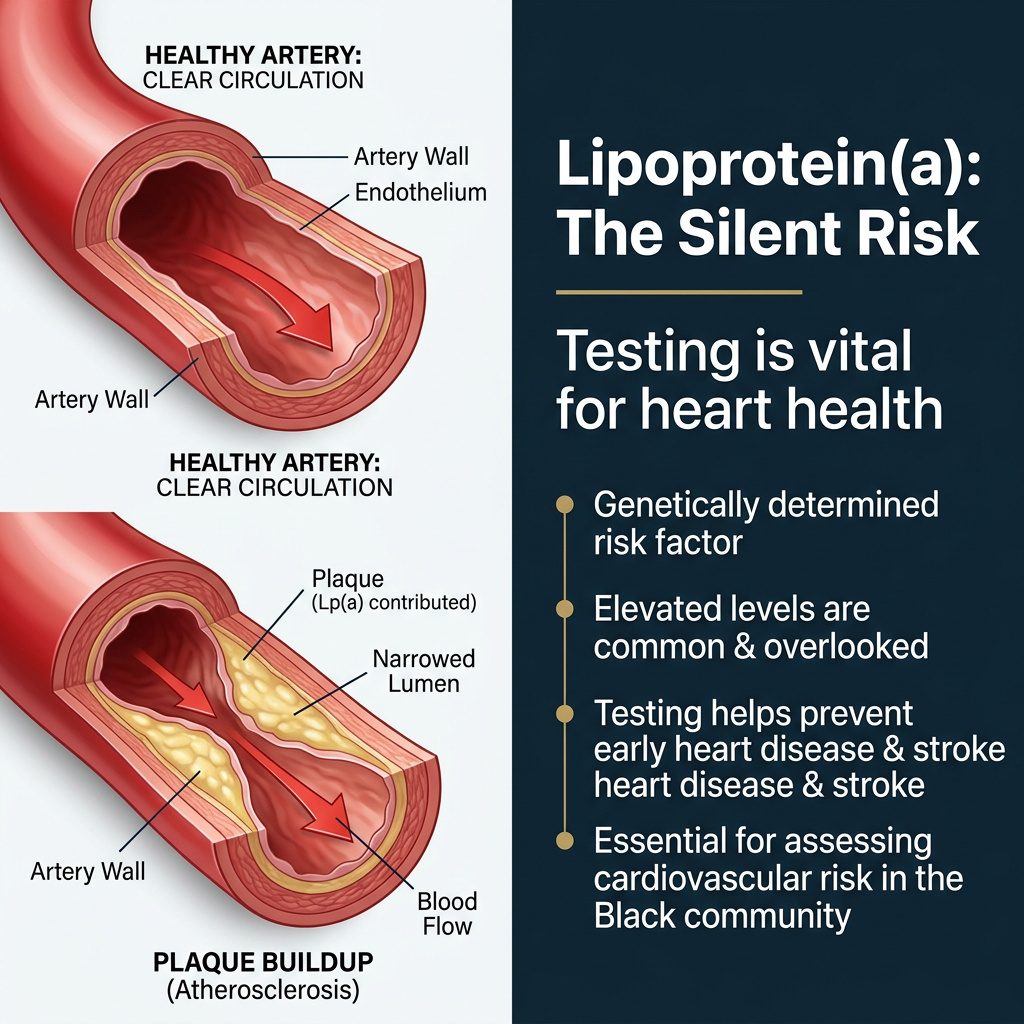
What Does Elevated Lp(a) Actually Do to Your Body?
Lp(a) damages your cardiovascular system through three main pathways:
1. It promotes atherosclerosis (plaque buildup). Lp(a) particles can enter the walls of your arteries, depositing oxidized fats that trigger inflammation and accelerate plaque formation. This leads to narrowing and hardening of the arteries.
2. It promotes blood clots (thrombosis). The apo(a) protein on Lp(a) structurally resembles plasminogen — a clot-dissolving protein in your body. Lp(a) competes with plasminogen and interferes with your body’s natural ability to break up clots, making dangerous blood clots more likely.
3. It promotes inflammation. Lp(a) carries oxidized phospholipids, highly inflammatory molecules that damage blood vessel walls and accelerate the development of heart disease.
The result? Elevated Lp(a) is linked to increased risk of:
- Heart attack (coronary heart disease)
- Ischemic stroke
- Peripheral artery disease
- Calcific aortic valve stenosis (a narrowing of the heart’s main valve)
Does Elevated Lp(a) Actually Increase Cardiovascular Risk in Black Americans?
For years, some researchers questioned whether elevated Lp(a) increased cardiovascular risk in Black Americans the same way it did in white Americans, partly because earlier studies were underpowered — they simply did not include enough Black participants to draw reliable conclusions.
The ARIC study settled much of this debate. After 20 years of follow-up, researchers found that elevated Lp(a) was indeed a statistically significant risk factor for cardiovascular disease in Black Americans. Specifically, for every standard deviation increase in Lp(a) levels:
- Risk of cardiovascular disease increased by 13%
- Risk of ischemic stroke increased by 21%
- Risk of coronary heart disease increased by 11%
The stroke risk finding is particularly significant. Black Americans already face a disproportionately high risk of stroke compared to white Americans, and Lp(a)’s especially strong association with ischemic stroke in our community makes this an even more urgent conversation.
One nuance worth understanding: because Lp(a) levels are naturally higher across the board in Black Americans, the risk threshold may differ. The level that signals elevated risk in a white patient may actually correspond to a much lower percentile in a Black patient. In other words, the same Lp(a) number carries different meaning depending on your racial background — and current guidelines have been slow to account for this.
You Can’t Treat What You Don’t Measure
Here is one of the most frustrating parts of this story: Lp(a) testing is performed far too infrequently, even in patients at high cardiovascular risk. Data from a large health system showed that fewer than 1% of eligible patients were even tested for Lp(a) levels.
And within that small group that did get tested, Black individuals were more likely to have established cardiovascular disease already present — meaning they were often only tested after heart disease had already set in. That is too late.
Who should be tested?
Major cardiology and endocrinology guidelines recommend Lp(a) testing at least once in adulthood for anyone who:
- Has a personal or family history of premature cardiovascular disease (heart attack or stroke before age 55 in men, age 65 in women)
- Has a family history of elevated Lp(a)
- Is of African ancestry or South Asian ancestry
- Has had a cardiovascular event despite normal LDL cholesterol levels
If you are Black, that means you likely qualify for Lp(a) testing simply based on your ancestry. Ask your doctor to check it. It is a simple blood test.
What Can You Do If Your Lp(a) Is High?
Here is where the news has been frustrating — but is becoming more hopeful. Standard cholesterol-lowering medications have little to no effect on Lp(a):
- Statins (like atorvastatin and rosuvastatin): Do not meaningfully lower Lp(a). In fact, some studies suggest statins may slightly raise Lp(a) levels.
- PCSK9 inhibitors (evolocumab, alirocumab): Powerful LDL-lowering drugs that offer modest Lp(a) reduction of 20–30%, but this is generally not enough for patients with very high levels.
- Niacin: Can lower Lp(a) modestly, but clinical trials have not demonstrated that this translates to fewer cardiovascular events, and it carries significant side effects.
So what do we do right now? Even though there is no approved drug specifically targeting Lp(a) yet, having a high Lp(a) level still gives you and your doctor critical information. It means you should:
- Aggressively lower your LDL cholesterol to reduce your overall cardiovascular burden
- Control blood pressure rigorously — especially important in the Black community where hypertension rates are already elevated
- Manage diabetes and blood sugar tightly
- Avoid smoking entirely
- Maintain a healthy weight
Think of elevated Lp(a) as a reason to be even more serious about every other risk factor you can control.
The New Wave of Lp(a)-Lowering Therapies: A Reason for Hope
This is where the medical landscape is changing rapidly, and Black Americans stand to benefit enormously. Several cutting-edge therapies are currently in advanced clinical trials, targeting Lp(a) directly:
RNA-based therapies (siRNA and ASO agents):
- Olpasiran, lepodisiran, and zerlasiran are small interfering RNA (siRNA) medications that block the liver’s production of Lp(a). Early trials have shown reductions in Lp(a) of 80–100% — dramatic results that would have seemed impossible just a decade ago. These are currently injected subcutaneously (under the skin) every few months. Major cardiovascular outcomes trials — including the OCEAN(a) and Lp(a) HORIZON trials — are underway to confirm whether these dramatic Lp(a) reductions translate to fewer heart attacks and strokes.
- Pelacarsen, an antisense oligonucleotide (ASO), also targets Lp(a) production in the liver and reduces levels by approximately 80%.
Oral therapy:
- Muvalaplin represents a major breakthrough as the first oral medication designed to lower Lp(a). It works differently — rather than blocking Lp(a) production, it disrupts the assembly of the Lp(a) particle itself. In a Phase 2 trial presented at the American Heart Association 2024 Scientific Sessions, muvalaplin lowered Lp(a) by up to 65% in patients at high cardiovascular risk. An oral pill taken daily would be transformative for patients who cannot or will not take injectable medications.
None of these therapies has received FDA approval yet as of this writing, but the clinical trial data are encouraging. Most experts anticipate approvals within the next few years. When they arrive, Black Americans — who carry the highest Lp(a) burden of any group — should be among the first to benefit.
What You Should Do Right Now
- Ask your doctor to test your Lp(a) level. It only needs to be done once in most circumstances, unless your kidneys decline or major hormonal changes occur (such as menopause). Simply say: “I’ve read that African Americans have higher Lp(a) levels and higher cardiovascular risk. Can we add an Lp(a) test to my next blood draw?”
- Know your number. Lp(a) above 50 mg/dL (or 125 nmol/L) is generally considered elevated and a risk enhancer. Levels above 180 mg/dL represent very high risk and may warrant specialist referral.
- Share your result with your family. Because Lp(a) is primarily genetic, if your level is elevated, your children, siblings, and parents may also have elevated levels. This is a family conversation worth having.
- Double down on what you can control. Keep your blood pressure, LDL cholesterol, blood sugar, and body weight in a healthy range. These are the levers you can pull today.
- Stay informed about clinical trials. If your Lp(a) is very high and you have cardiovascular disease or are at high risk, ask your cardiologist about clinical trial eligibility. Clinical trials for Lp(a)-lowering drugs are actively enrolling patients.
The Bottom Line
Lipoprotein(a) is one of the most powerful — and most overlooked — cardiovascular risk factors in the Black community. African Americans carry the highest Lp(a) levels of any racial group in the world, driven largely by genetic differences. We now know that elevated Lp(a) significantly raises the risk of heart attack and stroke in Black Americans, yet testing remains rare and awareness is low.
The good news is that a new generation of therapies is on the horizon that could dramatically lower Lp(a) levels. But the first step is knowing your number. Talk to your doctor about getting tested. Your heart — and your family’s hearts — may depend on it.